- pancreatic uncinate process activity,
- inflammation,
- osteoblastic activity, and
- splenosis.
- They also highlight the complementary role of (FDG) PET/CT, including the advantages of using both GaTate PET/CT and FDG PET/CT to evaluate sites of well- and poorly differentiated disease. The use of GaTate PET/CT together with FDG PET/CT allows identification of tumor heterogeneity, which provides prognostic information. It also allows optimal patient management, including theranostic application of peptide receptor radionuclide therapy, and the restaging of patients following therapy
Somatostatin, also known as SRIF (somatotropin release inhibiting factor) is an endogenous cyclic 14 amino acid polypeptide (SRIF-14, a tetradecapeptide). It was first identified by Krulich et al. in 1968...as an
This precursor contains a signal region of 24 amino acids, which targets the molecule for secretion and is subsequently removed. This leaves a 92 amino acid polypeptide called prosomatostatin which is processed enzymatically to generate SRIF-14 or SRIF-28. These two forms of somatostatin are differentially synthesised in a tissue-specific manner; for example, SRIF-14 was
found to be the predominant form within the hypothalamus and
amygdala, and equal amounts of the two were found in the median eminence.
They may involve different processing enzymes which are present in some cell types but not others, leading to a greater diversity of SRIF function .SRIF-14 and SRIF-28 have a wide distribution throughout the central nervous system as well as in
peripheral tissues, for example in the
pituitary,
pancreas and
stomach.
They have been found to regulate the secretion of various hormones as well as GH, such as thyroid-stimulating hormone (TSH), insulin and glucagon. Other effects of SRIF include modulation of cell proliferation and angiogenesis.The side effects of endogenous somatostatin are low due to it being produced and inactivated around the local sites of action.
Somatostatin receptors have a very widespread distribution throughout the brain and peripheral tissues. mRNA of all the 5 subtypes has been found within the human and rodent brain, differentially distributed among regions such as the
cerebral cortex
cerebellum
cerebrum
pituitary
hippocampus
hypothalamus
thalamus
amygdala
striatum [ and olfactory bulb ]
The SST5 receptor is less abundant in the brain than the other subtypes. Other areas of the body where somatostatin receptor mRNA and/or protein has been found include:
the pancreatic islets
intestine ,
stomach
lung
kidney,
liver ,
jejunum
spleen ,
skeletal muscles
heart retina], blood vessels, placenta and in some elements of the peripheral nervous system (myenteric and submucosal plexus, Cajal cells)
Somatostatin receptors are also expressed in tumours in peritumoral vessels and various blood cells.
A range of other tissue functions of somatostatin, acting through the 5 somatostatin receptors, has been found. These include:
modulation of glucagon secretion
insulin secretion,
cell proliferation
gastric acid secretion
, angiogenesis
peristalsis in the jejunum
and neuronal activity
There is evidence that SST1 is an auto receptor in the retina, modulating SRIF levels . The development of somatostatin receptor knock-out mice has given further evidence towards the functions of the receptors.
Somatostatin released from the hypothalamus activates somatostatin receptors located within the anterior pituitary to cause inhibition of GH secretion . Somatostatin works alongside another hypothalamic regulatory hormone, GHRH (growth hormone releasing hormone), to regulate a pulsatile GH release before acting on peripheral tissues and endocrine organs to regulate cell growth. Feedback mechanisms are present in order to regulate GH secretion: for example, GH can stimulate insulin-like growth factors (IGF-I and IGF-II) that can stimulate SRIF secretion from the hypothalamus . SRIF can also regulate its own release via autoreceptors, thought to be the SST1 subtype . Knock-out mice showing the physiological effects of removal of somatostatin receptor subtypes confirm these effects on GH secretion .
The anti-proliferative effects of somatostatin are due to a negative control of cell growth, of both normal cells and tumours.
Somatostatin has also been shown to inhibit the growth and proliferation of blood vessels (angiogenesis), by inhibition of endothelial cell growth, resulting in an inhibition of tumour cell growth. Inhibition of angiogenesis has been shown to be via the SST3 receptor subtype, and involve inhibition of MAPK and endothelial nitric oxide synthase (eNOS- Endothelial nitric oxide synthase is a key enzyme in production of the vasodilator, nitric oxide (NO) . ) activity.
The highest- intensity physiologic uptake of GaTate is seen in the
- spleen, followed by the
- adrenal glands,
- kidneys, and
- pituitary gland.
Moderately intense uptake is also seen in the- liver,
- salivary glands, and
- thyroid gland. This biodistribution reflects a combination of specific receptor binding and nonspecific tissue handling of the peptide.
Uptake in the- endocrine organs,
- salivary glands, and
- spleen is mediated by expression of SSTR,
- whereas uptake in the kidneys and liver is not.
The peptide is small enough to be filtered through glomeruli but is also partially reabsorbed in the proximal convoluted tubule, resulting in high activity in the collecting system and bladder as well as retained activity in the renal parenchyma. Variable physiologic uptake in the small and large intestine and gastric activity are seen; the exact mechanism of this uptake is unclear but may reflect variable degrees of neuroendocrine cell hyperplasia, since the appearance of the uptake is generally too rapid to reflect gastrointestinal excretion. Pathologic uptake can be graded with a semiquantitative visual scoring system that consists of a scale from 0 to 4 and uses the liver and spleen as reference organs. This scoring system is named after Eric Krenning, who pioneered SSTR imaging at the Erasmus Medical Center in Rotterdam, the Netherlands. Although Krenning originally designed his scoring system for planar octreotide imaging, we have found it to be a valuable descriptor for reporting. Compared with (FDG) PET/CT, there is minimal background activity in soft tissue and muscle, which contributes to high tumorto-background contrast at pathologic sites. The combination of low background and high tumor uptake also contributes to a “sink effect,” whereby physiologic uptake, particularly in the spleen and liver, is reduced in patients with a high burden of disease . Uptake at physiologic and pathologic sites may change in patients who undergo concomitant short- or long-acting somatostatin analog therapy, which competes with the radiotracer for
Somatostatin is a known regulator of insulin and glucagon secretion (which control glucose homeostasis) from pancreatic islets . Beta cells of the pancreas secrete insulin and contain mainly SST5 receptors. Alpha cells of the pancreas secrete glucagon and contain mainly SST2 receptors. SST2 and SST5 receptor knock-out mice affirm these effects.
Somatostatin, released from cells located in the stomach, potently inhibits gastric acid secretion through inhibition of histamine release and through direct inhibition on parietal cells [35]. This is not shown in SST2 receptor knock-out mice despite it having been shown that the effects of peripheral somatostatin on gastric acid secretion are via the SST2 subtype. This suggests there are somatostatin-independent mechanisms compensating for the lack of inhibitory input by somatostatin . Another study involving SST2 knock-out mice shows that somatostatin suppresses gastric acid secretion via the SST2 receptor subtype, by inhibiting the actions of gastrin.
The SST1 receptor is an autoreceptor in the rat retina, modulating SRIF levels. This has been confirmed using SST1 knock-out mice, where there was an increase in SST levels accompanied by up-regulation of the SST2 receptors. In SST2 knock-out mice there was a reciprocated up-regulation of SST1 receptors and consequently a decrease in SRIF levels due to SST1 acting as an auto receptor.
Activation of somatostatin receptors is known to result in the
- inhibition of peristalsis in the jejunum, and knock-out studies provided evidence of SST2-mediated as well as non-SST2-mediated constituents of this inhibition
- Analysis of peptide–receptor interactions provides insights for understanding functions of proteins in cells. In this work, we report the development of a fluorescent biosensor for the analysis of peptide–receptor interactions using graphene oxide (GO) and fluorescein isothiocyanate (FITC)-labeled octreotide (FOC).
Octreotide is a synthesized cyclic peptide with somatostatin-like bioactivity that has been clinically employed. FOC exhibits high adsorption affinity for GO, and its binding results in efficient fluorescence quenching of FITC. Interestingly, the specific binding of the antibody anti-octreotide (AOC) with FOC competitively releases FOC from the GO surface, leading to the recovery of fluorescence. By using this GO-based fluorescent platform, we can detect AOC with a low detection limit of 2 ng/mL. As a step further, we employ this GO–FOC biosensor to image somatostatin receptor subtype 2 overexpressed AR42J ( AR42J cells derive from azaserine-induced malignant nodules from the rat pancreas) tumor cells, which demonstrates high promise for molecular imaging in cancer diagnosis.
Somatostatin receptors (SSTRs) are present on the cell surface of neuroendocrine cells, providing a unique and specific molecular target for imaging. Somatostatin is a peptide hormone that binds to this receptor, thereby regulating neurotransmission, hormone secretion, and cell proliferation. Somatostatin generally exerts an inhibitory effect such as suppressing the release of pancreatic hormones or reducing smooth muscle contractions.
NETs arising from the gastrointestinal tract and pancreas are a heterogeneous disease with many different subtypes, ranging in aggressiveness from very indolent tumors that progress over decades to highly aggressive malignancies. Both indolent and highly aggressive tumors have the propensity to metastasize, and indolent tumors can cause significant morbidity if they secrete bioactive hormones. These hormones can result in a variety of clinical syndromes, such as carcinoid syndrome
Prominent islet cell clusters or islet cell hypertrophy can also occur elsewhere, resulting in heterogeneous low-grade pancreatic uptake. Mistaking exaggerated physiologic pancreatic uptake for pancreatic tumor can result in harmful consequences for the patient, especially if a Whipple procedure is performed on the basis of these findings. Close correlation with findings at MR imaging and thin section multiphase CT can be helpful in further assessing equivocal findings.
Spleen.—Splenectomy is commonly performed in patients with pancreatic NET owing to the proximity of the spleen to the distal pancreas and the necessity of excising it when performing en bloc resection of the pancreatic tail. Splenosis is a common finding at restaging, and nodular splenosis can be mistaken for peritoneal metastases at anatomic imaging and GaTate PET/CT because, like the normal spleen, these nodules demonstrate very intense uptake. Thus, particularly in patients who undergo interval splenectomy, intense uptake in new, well-defined, round, peritoneal soft-tissue nodules may be due to splenosis. If there is uncertainty, denatured red blood cell SPECT/CT can help further characterize such lesions. In patients who do not undergo splenectomy, 80% of accessory spleens occur at the splenic hilum, although they may arise anywhere in the peritoneal cavity or within the pancreas. Splenunculi have lower-intensity uptake than the spleen (SUVmax ≅11 versus 29 for the spleen) (28), which may reflect a higher delivery rate of the peptide to the spleen due to its high arterial blood flow. Intrapancreatic splenunculus is another potential cause of false-positive GaTate PET/CT findings.

Pheochromocytoma and Paraganglioma Early experience with octreotide imaging demonstrated high uptake in neuroectodermal tumors, including pheochromocytoma and paraganglioma . Subsequently, iodine --metaiodobenzylguanidine (MIBG) became more commonly used in many centers for functional imaging. Our early experience with GaTate PET/CT suggests that it is the functional imaging modality of choice, and it has rapidly become our standard of care. In a small series of 12 patients with metastatic disease,
The EANM 2012 guidelines for radionuclide imaging of pheochromocytoma and paraganglioma provide a complex system involving selective use of 123I-MIBG, fluorine 18 DOPA, FDG, 111In/68Ga SSTR, or 18F-fluorodopamine, depending on genetic status and test availability . Our experience suggests that GaTate PET/
CT is highly accurate across the range of mutations, including SDHx mutations, von Hippel– Lindau (VHL) mutations, multiple endocrine neoplasia type 2 (RET) mutations, and neurofibromatosis type 1 (NF1) mutations . In contrast, other functional tests demonstrate uptake only in certain phenotypes. For example, FDG PET/CT demonstrates high uptake in SDHx-related disease owing to dysfunction of mitochondrial oxidative phosphorylation, but it typically demonstrates low uptake in RET/NF1related disease. The high uptake of GaTate across the spectrum of disease suggests that GaTate PET/CT may be the best first-line investigation. MIBG SPECT/CT remains useful in assessment.
Inflammatory Processes
White blood cells including leukocytes and macrophages express SSTR 2, and some researchers have used this phenomenon to help image inflammatory processes such as atherosclerotic plaques with SSTR PET/CT (33). Inflammatory uptake is invariably low or very low grade and is most commonly seen in reactive hilar, mediastinal, axillary, or inguinal nodes. Inflammatory uptake is also commonly observed in prostatitis or post–radiation therapy change, although any inflammatory process may demonstrate some GaTate activity.
Meningioma Tiny incidental meningiomas are frequently visualized at GaTate PET/CT performed for other reasons (Fig 14). These subcentimeter lesions do not require further investigation but highlight the exquisite sensitivity and utility of GaTate PET/CT for the detection and characterization of meningioma. In a recent study of 134 patients, GaToc PET/CT was found to be superior to contrast-enhanced MR imaging, with 190 meningiomas being detected at PET compared with 171 at contrast-enhanced MR imaging.. Furthermore, with knowledge of the PET/CT data, the MR imaging abnormalities could be visualized at only four of 19 sites (42). Tumors adjacent to the falx cerebri at the skull base or obscured by imaging artifacts or calcification were particularly difficult to visualize at MR imaging . Moreover, GaTate PET/CT is highly specific in characterizing abnormalities and is therefore useful if there is uncertainty as to whether an MR imaging finding represents a meningioma. In larger anaplastic meningiomas, the boundaries of involvement can be clearly defined at GaTate PET/CT . There is an increasing role for GaTate PET/CT or PET/MR imaging in improving the delineation of gross tumor volume for radiation treatment planning ., often leading to a reduction in treatment volume compared with MR imaging or CT. There is also evidence that GaTate PET/CT can improve outcomes by helping identify patients who are likely to benefit from PRRT ..
Other Tumors
- There are a number of other tumors with variable SSTR expression in which GaTate PET/CT has a role in both imaging and the evaluation of suitability for PRRT. These tumors include, but are not limited to, medullary thyroid cancer,
- Merkel cell carcinoma, small cell carcinoma, esthesioneuroblastoma , and iodine-negative thyroid cancer. The utility of GaTate PET/CT in other tumors has yet to be explored.
Conclusion
GaTate PET/CT has an array of clinical applications in gastroenteropancreatic and other NETs, in which it is proving to represent a new standard of reference given its superior accuracy compared with conventional imaging techniques. The strength of GaTate PET/CT lies not only in its high sensitivity, but also in its ability to characterize whole-body SSTR expression, which confers a high specificity. This allows the selection of patients with metastatic disease for hormonal therapy or PRRT. FDG PET/CT plays a complementary role by helping identify sites of poorly differentiated disease on the basis of their higher proliferation rate. In selected patients, the use of both techniques can elegantly demonstrate tumor heterogeneity, which can be pivotal in guiding biopsy and selecting optimal management for individual patients.
- Oncogenic Osteomalacia--Oncogenic osteomalacia — also referred to as tumor-induced osteomalacia (TIO) — is a rare endocrine disorder in which a small bony or soft tissue mesenchymal tumor causes hypophosphatemia via secretion of FGF23. The latter causes hypophosphatemia via two mechanisms: 1) reduction of renal tubular phosphate reabsorption leading to phosphaturia, and 2) impairment of hydroxylation of 25-hydroxyvitamin D to 1,25-dihydroxyvitamin D, thus reducing intestinal phosphorus absorption. As a result of chronic hypophosphatemia, patients develop osteomalacia and associated insufficiency fractures.
- Neuroblastoma A cancer that is commonly found in the adrenal glands.Neuroblastoma is a cancer often found in the small glands on top of the kidneys (adrenal glands). It can develop in the stomach, chest, neck, pelvis and bones. Children aged five or younger are most commonly affected.
68Ga-DOTATATE PET/CT provides incremental diagnostic information compared to Octreoscan, MIBG scintigraphy and conventional imaging. 68Ga-DOTATATE also has been proved to have significant impact in management of patients with neuroendocrine tumors. Additional benefit of 68Ga-DOTATATE PET/CT include patient convenience with short time acquisition and lower radiation exposure signifying the important role of 68Ga-DOTATATE/CT in clinical practice of neuroendocrine and other somatostatin-avid malignancies.
How aggressive is the growth of the tumour?
This is where the doctors understand the progression or the stability of the tumour. This is an important parameter that doctors need to understand. If the tumour is stable and the patient is fairly asymptomatic, doctors recommend to wait and watch. And if the tumour is progressing and is spreading to other sites, doctors recommend PRRT as the recommended mode of treatment.
To determine whether the tumour cells are showing a good receptor expressions that can be used for targeting PRRT, doctors ask for a Gallium 68 Dotanoc Scan or an Octreotide PET CT. A Gallium 68 Dotanoc whole body scan is a type of PET CT that is specifically done for neuroendocrine tumours. Apart from this scan, doctors might also look at a Technetium Hynic-TOC Scan that also looks at the receptors.
Further, doctors also ask for a regular FDG PET CT so as to determine the aggressiveness of the tumour. This FDG PET CT also helps doctors on the prognosis of the condition – if the neuroendocrine tumour shows positive on the FDG PET CT scan, then doctors know that the condition of the patient is less likely to benefit from PRRT.
Neuroendocrine tumors (NETs) are a rare group of neoplasms with an incidence of about 35 cases per 100,000 people in the United States. The defined characteristic of NETs is the expression of somatostatin receptors (SST) . This unique feature has enabled the field of nuclear medicine and molecular imaging to image these tumors with radiolabelled somatostatin analogues agent. Octreotide, a long-acting somatostatin analogue, was initially used in 1989 and since then it evolved as an important agent in the initial evaluation and management of NETs using molecular imaging technique
"I am not sure what metastatic NET you are talking about. Your haemangiendotheliomas have always expressed dotanoc uptake.
Somatostatin receptors may be over expressed in a myriad of diseases. Does not necessarily mean you have metastatic NET. And whether PRRT is the treatment for you or not needs to be assessed."said the doctor.
Current findings




- Hoarseness
- Breathy voice
- Being unable to speak loudly
- Limited pitch and loudness
- Being able to produce voice for a very short time
- Choking or coughing while eating
- Possible pneumonia if food and liquid get into the lungs. This may happen if the vocal folds cannot close to protect the airway while swallowing.
There's no reason for my choking and hoarse voice.
- I can't stand fall
- I vomit suddenly
- I have neck pain and headaches
- Swallowing problem.
I got choked on solid food and coughed my lungs out.
I bite my tongue while eating or speaking and the dentist said to use lidocaine
My right leg knee feels the same kind of electricity as TN. My gait and I bumped into the bookshelf
My right leg has become weak and if you touch I fall
I am confused because of symptoms of the pancreas and brain. I am going to the toilet after every meal.
I am going for a PET scan with..I am bothered about what to do with my brain. The doctor said my right side trigeminal neuralgia is the same. I don't agree. I took the highest dose of tegretol, and pregabalin, noresthiterone, gabapentin but when I couldn't tolerate I got the cyberknife. I am on no medicine now I have maxillary and mandibular numbness not always. I have pain from the neck which goes behind the ears.
Size is the main criteria for determining approximate risk level for pNETs. Tumors that are greater than, or equal to, 3 cm should be considered high risk and be evaluated for surgery. pNETs with a diameter between 1.2-1.5 cm and 3 cm should be considered moderate risk and be monitored closely. Those smaller than 1.2-1.5 cm are considered low risk. The location of the tumor within the pancreas should also be taken into consideration, as tumors in the head of the pancreas are typically removed when they are smaller to allow for less extensive surgeries.
"If I have decided to do a particular scan for you in a particular way, that is after a lot of thought and deliberations. Dont you dare question my competence. I have listened to enough nonsense from you. Dont dare to send me any such rubbish message again in the future" said a doctor full of enthusiasm for the patient.


While it is generally accepted that stage IV (presence of metastasis) portends a poor prognosis for most neoplasms including NENs, there is no consensus on the gravity and importance of metastatic sites, or how they interplay with the primary tumor site when it comes to survival estimates.
Good morning. My trip to the bathroom. I am a Bengali and eat spicy food.
No ma'am I eat mostly fish and chicken soup and such things. I can't go twice. and kindly don't repeat I am playing the doctor. Every patient has the right to know. Knowledge isn't anyone's property.
This score emphasizes the importance of metastatic location and shows that brain and liver involvement carry a higher risk of death regardless of other wellknown factors, such as origin of the tumor or histology.

Who created
Hardly get any support from my country, I believe, I was born in a wrong country as my tuition teacher said eons ago.
The medical profession many self-centred egoistic people that think they know everything and all patients should just shut up and be grateful and any questioning of their ability or judgement is met with intense anger.. metastatic net cancer Showing their true colours.
There are 2 tumours causing my hearing loss one in the connection between the two halves of brain and one is growing and growth needs to be stopped. All tumours if treated won't grow. New ones if occur need to be watched but I don't think after chemotherapy will occur. I need an appointment.
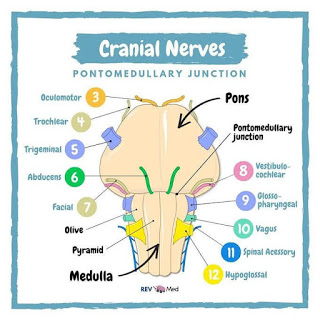
The facial nerve (VII) is a mixed one, considering its motor root in association with the sensitive root given by the intermediate (Wrisberg) nerve1. The taste of the anterior two-thirds of the tongue on each side are its responsibility. From the tongue, this afferent, pre-ganglionic route follows through the lingual nerve (association of nerves V and VII), and afterward through the tympanic cord nerve (facial branch), to make synapses on the geniculate ganglion. Through the intermediate nerve, the postganglionic fibers (afferent visceral special - gustative route) synapse in the solitary tract nucleus of the medulla oblongata, associated with the general afferent visceral fibers, providing sensitive innervation to the mucosa of the nasal cavities and soft palate.
The parasympathetic efferent fibers of the facial nerve, originating from the upper salivary nucleus located on each side of the upper portion of the medulla oblongata, run through the intermediate nerve and afterward through the tympanic cord nerve to make synapses in the submandibular ganglion. Thence, through postganglionic fibers, they stimulate salivary secretion of the submandibular and sublingual glands.
The motor portion of the facial nerve has its nucleus on the ventral portion of the pons. Its fibers stimulate the skin-inserted muscles in the face, neck, and scalp, as well as the posterior belly of digastric and stylohyoid muscles.
Symptoms of a NET
experience the following tumor-related symptoms or signs:
My
Fatigue
Loss of appetite
Unexplained weight loss
Symptoms related to the tumor size and/or location:
Persistent pain in a specific area
Thickening or a lump in any part of the body
Nausea or vomiting
A cough or hoarseness that does not go away
Changes in bowel or bladder habits
Jaundice, which is the yellowing of the skin and whites of the eyes
Unusual bleeding or discharge
Symptoms related to the release of hormones:
Diarrhea
Facial flushing, usually without sweating
Hyperglycemia, which is a high level of glucose in the blood. Glucose is a sugar that is converted into energy by the body. Hyperglycemia causes frequent urination, increased thirst, and increased hunger.
Hypoglycemia, which is a low level of glucose in the blood. It causes fatigue, nervousness and shakiness, dizziness or light-headedness, sweating, seizures, and fainting.
Ulcer disease
Skin rash
Confusion
Anxiety
The symptoms caused by a somatostatinoma may include the following:
pain in the abdomen (most common symptom)
diabetes
unexplained weight loss
gallstones
steatorrhea, or fatty stools
bowel blockage
diarrhea
Peripheral effects of serotonin are local vasoconstriction where it is released and also vasodilatation and increased capillary permeability; constriction of veins and induction of venous thrombosis and promotion of platelet aggregation.
Serotonin has a positive chronotropic effect on the heart through 5HT4 receptors and can cause cardiac rhythm disorders.
• Excessive serotonin gives rise to debilitating diarrhea affecting the quality of life of patients with carcinoid syndrome.
• Prolonged exposure to high level of serotonin can cause fibrosis of heart valves, more commonly on the right side,
causing valvular heart disease. Excessive serotonin is also linked to fibrosis of uterus, skin (scleroderma),
pulmonary and retroperitoneal fibrosis in the long run,causing multiple complications.
Low levels of serotonin are often associated with many behavioral and emotional disorders.
10 months of diarrhea wore me out.

Maryfilomena E Rita Viñcenza I am honoured by your comment
"Payel Bhattacharya you are what I call a beautiful soul . You see, I knew !!!! I see such light coming from you . There is a special reason why God saved you and uses you for his glory . I am so honored to have Met you . May God bless you . You have lightened up my mind and spirit ; you see , it is 20 years from 9/11, my love of my life Til death did we part , Mark , died from being a first responder a NYPD Sgt , who got kidney cancer from working months there . This puts my gift of life into perspective once again . I like you always chose to find the flowers the birds the breeze the music in life in the lil moments of the day . I have lost so much of my light since Mark died nearly 8 years ago . This is how I have written poems in the past and more importantly how I have spoken to encourage and enlighten others in their dark moments . Thank you . I’ll pray blessings over you . 💝"
I am happy to have a great friend too. I hardly got any good words or support from Indians
Friendship is one of life's greatest treasures.
Souls connected in space and time beyond any measure
Even if we don't see each other for years
Emotions yet untold;
As time goes on, and bonds grow strong,
They will all unfold.
You are a great friend and I am happy. Pray I get over it
Next story would be of a metastatic up-to-date yet ignorance drips from it.
After completing their medical degrees do they plunge into the world of unique diseases, keep themselves updated, keep track of all those maladies?
Knowledge is power, ignorance about your disease will lead you nowhere. I have come across a few such patients with inadequate and volatile knowledge and they haven't survived after the second surgery. Ah! Don't look at me in dismay!
If you have watched the '3 idiots' movie one of the Hindi movies I watched, I watch Tom Cruise, Robert Downey Jr, witty and action in English where things are on the edge but I liked this one. You can never learn from a book by memorizing it. Real knowledge is understanding the phenomenon. I grew up reading Carl Sagan and I admire science and I always have a question in my mind. Indians are always showing their true colours But I have never seen any other country so I don't know except whatsapp or zoom chat with them medical profession has many self-centred egoistic people that think they know everything and all patients should just shut up and be grateful and any questioning of their ability or judgement is rare... Who am I a mosquito but it's the goodness that makes the world spin. And we feel the bright sun will bring good tidings. There is positivity similarly there is negativity and both balance the world.
"Please block me..I will be very grateful. That gives u the option of unblocking me shud u ever need urgent help" said that abusive doctor.