

I had a subtotal thyroidectomy in 2006 for multi-nodular thyroid leading to goitre with retro-sternal extension. It was one of the longest surgeries lasting for 6 whole hours.
In a routine ultrasound of the neck on May 14th 2014, it was found…
"Left lobe of thyroid is not visualised (postoperative).
Remnant of the right lobe measures 5.2x8.9 mm. Adjacent to it at least 4 hypoecohypoecoic nodules seen measuring 6.2 mm, 10.8 mm, 11.5mm, and 12 mm in size with increased vascular flow within as well as at the periphery on CDF1 images. These are suggestive of hemangioblastomas in a known case."

It is critically important for the thyroid surgeon to employ strategies for minimizing and preventing hypoparathyroidism (or Hypopara for short), including carrying out the most appropriate extent of thyroidectomy for a specific patient.
The most straightforward way to avoid HypoPara is to limit the extent of thyroidectomy to a unilateral approach. Though the historical rationale for a “near-total” or “subtotal” thyroidectomy, instead of a total thyroidectomy, is in part preservation of the parathyroid glands, it has never been adequately studied whether this actually reduces the risk of HypoPara.
Parathyroid insufficiency, or relative HypoPara, may occur after central neck surgery and typically is manifested by clinical symptoms of HypoPara that require medical treatment, despite measured laboratory values within normal ranges. Transient or temporary HypoPara is defined as occurring for less than 6 months after surgery, while permanent HypoPara continues beyond 6 months after surgery.
The normal parathyroid function requires a rich blood supply; a normal parathyroid gland is composed of up to 30% capillary cells. Parathyroid blood supply is both delicate and complex and requires close attention during thyroidectomy to ensure its preservation. While the inferior thyroid artery is typically the dominant blood vessel that supplies the parathyroid within the thymo-thyroid cord (ligament) can dominate in some individuals.
Impaired PTH secretion results in postoperative hypocalcemia, through inhibition of bone resorption, reduction of 1,25-dihyroxy vitamin D synthesis by the kidneys, and reduced intestinal absorption of calcium.
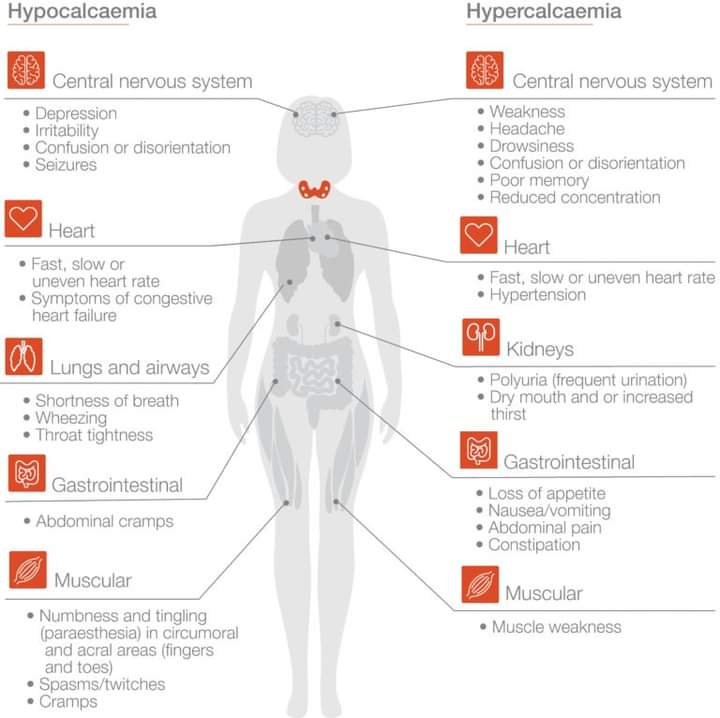
Symptoms and Signs
Hypocalcemia causes
neuromuscular excitability and cardiac electrical instability due to a reduced nerve and muscle cell depolarization threshold.
It's most common early symptoms are paresthesias, or numbness and tingling, of the perioral region and the fingertips. Muscle stiffness, cramps, and spasms are also common.
Neuropsychiatric symptoms include confusion, anger, depression, lightheadedness, and irritability. More sustained muscle contraction may lead to laryngospasm, and more severe neural excitability may lead to seizures.
Signs of hypocalcemia include observed or elicited tetany. Classic bedside findings are a positive Chvostek sign (facial muscle twitching upon tapping the preauricular region over the facial nerve; present at baseline in up to 25% of people), or a positive Trousseau sign (flexion of the wrist, thumb, and metacarpophalangeal joints and hyperextension of the fingers, upon brachial artery occlusion by inflation of a blood pressure cuff above systolic blood pressure).
Cardiovascular signs observed with progressive hypocalcemia include prolongation of the QT interval that can result in torsades de pointes, a form of ventricular tachycardia that may degenerate into ventricular fibrillation.
Acute symptoms may range from subtle to profound, and fortunately recognizable symptoms of mild to moderate hypocalcemia usually precede more life-threatening complications of severe hypocalcemia.

Calcium as total or ionized calcium blood levels are the mainstay of clinical monitoring. However, consideration of Vitamin D and magnesium levels is also necessary.

Hypoparathyroidism is a rare endocrine condition in which insufficient or inactive levels of parathyroid hormone (PTH) are produced by the four tiny parathyroid glands in your neck.
It may be due to a congenital, genetic, or autoimmune disorder that affects the function of the parathyroid glands or, more commonly, it may occur as the temporary or permanent result of surgery to the neck where there is removal or damage to the glands.
Insufficient PTH leads to low calcium levels in the blood, or hypocalcaemia. It causes electrolyte imbalance and can be a life-threatening condition if untreated.
Why is calcium so important? Calcium is vital to life and affects every cell in the body. Most people know about teeth and nails in connection with calcium but its effects are on the whole body - nerves, muscles, and organs. It helps blood to clot and is important in energy production. Calcium is crucial to us which is why the body has special mechanisms like the parathyroid glands to keep calcium levels constant.
Treatment with vitamin D analogues and calcium supplements is not ideal and can lead to long term renal problems. Calcium levels fluctuate but home calcium testers are not available so monitoring this condition can be challenging. Until 2015, Hypopara was the only endocrine condition without its own replacement hormone. Injectable parathyroid hormone is now licensed for use in the treatment of hypopara in the USA but is not yet available elsewhere.
No comments:
Post a Comment