Symptoms of a lung NET
There are 2 ways in which a lung NET can cause symptoms. A tumor itself can block the airway, causing a cough or shortness of breath. Or, hormones released by the tumor can cause carcinoid syndrome (see below). A lung NET is much less likely to cause carcinoid syndrome than a GI tract NET.
People with a lung NET may experience the following symptoms or signs:
Cough, with or without bloody sputum or phlegm
Wheezing
Post-obstructive pneumonia, which is when a tumor blocking a large air passage causes an infection
Chest pain
Carcinoid syndrome
Carcinoid tumor is a rare, slow-growing neuroendocrine tumor that accounts for less than 1% of all lung tumors. It occurs most commonly in the midgut, then the lung, and usually presents as a solid lesion. A patient has been reported with a typical carcinoid tumor that had undergone cystic degeneration.
Carcinoid tumors of the lung are a subgroup of neuroendocrine tumors of the lung, of lower grade than small cell carcinoma of the lung and large cell neuroendocrine carcinoma of the lung.
For a general discussion, please refer to any article on carcinoid tumors.
Pathology
Classification
Carcinoid tumors can be divided into two groups dependent on location:
Bronchial carcinoid tumors: central lesions
Peripheral pulmonary carcinoid tumors: peripheral lesions
Carcinoid tumors also can be divided into the two groups dependent on histology (requires resected specimen rather than biopsy ) as follows:
Typical carcinoid tumors of the lung
some reports describe this type as being more common 5
low grade/well-differentiated 4 atypical carcinoid tumors of the lungless well-differentiated
more aggressive
Cystic lung cancers are predominantly adenocarcinomas in about 80% of cases, with squamous cell carcinomas as the second most common subtype.
A rare number of other tumor types like adenosquamous, neuroendocrine, and lymphoma have been reported.
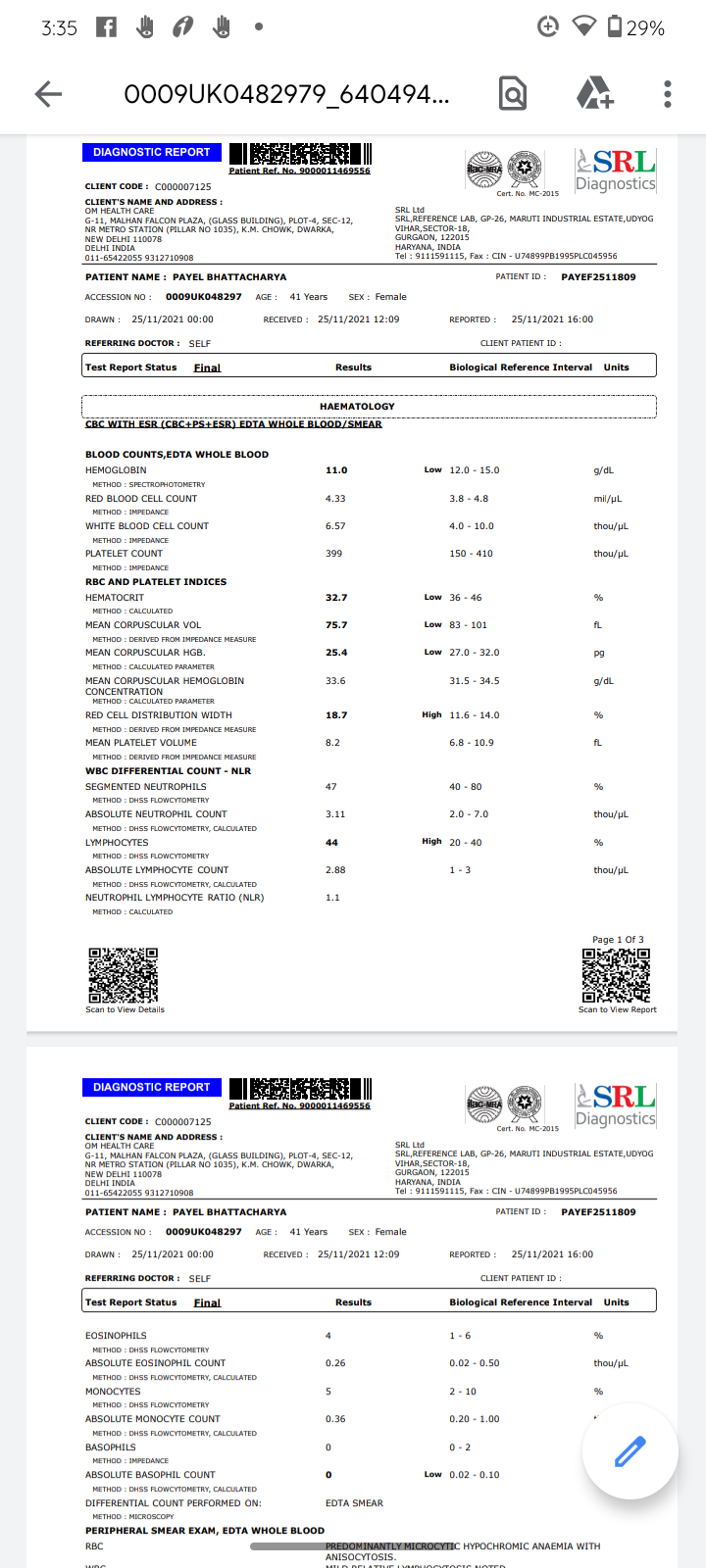
MILD RELATIVE LYMPHOCYTOSIS NOTED . Where platelets are supposed to be max 400 mine is 399Strong evidence has been accumulated since the beginning of the COVID-19 pandemic that neutrophils play an important role in the pathophysiology, particularly in those with severe disease courses. While originally considered to be a rather homogeneous cell type, recent attention to neutrophils has uncovered their fascinating transcriptional and functional diversity as well as their developmental trajectories. These new findings are important to better understand the many facets of neutrophil involvement not only in COVID-19 but also many other acute or chronic inflammatory diseases, both communicable and non-communicable. Here, we highlight the observed immune deviation of neutrophils in COVID-19 and summarize several promising therapeutic attempts to precisely target neutrophils and their reactivity in patients with COVID-
19
My past COVID has no reIationship with my lung problems here.
Multiple underlying histopathologic substrates (eg. focal tumor proliferation, fibrosis, lepidic tumor growth along alveolar walls, emphysema) relate to the imaging features of cystic lung cancer and are responsible for either the solid component, septations, ground glass, and cystic air spaces.
The most widely quoted mechanism of air space formation is “check-valve” ventilation.
The air can enter in inspiration but cannot return during expiration due to partial obstruction of the terminal airway proximal to the cystic air space due to tumor cells and fibrosis.
This leads to development, persistency, and enlargement of the cystic air space.
My Findings:
CHEST:
Multiple ill-defined calcified & non-calcified nodules are seen scattered in both lungs, predominantly in
upper lobes, largest measuring 2x1.3 cm in the right upper lobe.
A thin-walled cyst in the left upper lobe. Trace centriacinar emphysema in the left upper lobe. Centriacinar emphysema, is a long-term, progressive lung disease hence the FDG done without contrast to expose me to more radiation there studying the lungs in detail was neglected.
The rest of the bilateral lungs are normal in attenuation.
Trachea and mainstem bronchi are normal.
Major mediastinal vessels are normal.
Few calcified sub cm mediastinal lymph nodes. No enlarged mediastinal lymph nodes.
No pleural/pericardial effusion is seen. Bone window shows no significant abnormality.
Note is made of a few sub cm calcified foci in bilateral breasts.
Breast calcifications are calcium deposits within the breast tissue. They appear as white spots or flecks on a mammogram etc.
Breast calcifications are common on mammograms, and they're especially prevalent after age 50. Although breast calcifications are usually noncancerous (benign), certain patterns of calcifications — such as tight clusters with irregular shapes and fine appearance — may indicate breast cancer or precancerous changes to breast tissue.
Some patients may have several years’ delay in the correct diagnosis due to misdiagnosis as asthma. I am a victim of misdiagnosis.Like other neuroendocrine tumors, lung carcinoids may secrete hormones. Endocrine symptoms are however rare. Despite serotonin, immunoreactivity is present in up to 84% of the tumors.
With dry cough and
progressive dyspnea ( Shortness of breath)
I get to know CHEST:
"Multiple ill-defined calcified & non-calcified nodules are seen scattered in both lungs, predominantly in
upper lobes, largest measuring 2x1.3 cm in the right upper lobe.
A thin-walled cyst in the left upper lobe."
Early lung cancers associated with cystic airspaces are increasingly being recognized as a cause of delayed diagnoses—owing to data gathered from screening trials and encounters in routine clinical practice as more patients undergo serial imaging. Several morphologic subtypes of cancers associated with cystic airspaces exist and can exhibit variable patterns of progression as the solid elements of the tumor grow.
It was identified and assessed 30 lung cancers from a total of 2954 primary lung cancers diagnosed at their institution. In these 30 cases, cysts were in or adjacent to the cancers at some point leading up to the histologic diagnosis. In 20% of the cases, the cystic airspace was multilocular when it was first identified. Twenty-five percent of the remaining cystic airspaces that were unilocular at first visualization evolved to have a multilocular appearance over the course of observations. None of the initially multilocular lesions evolved to have a unilocular morphology.
Lung cancers arising from bullous emphysematous disease also are the subject of a number of anecdotal case reports, as well as a study whose results indicated “poorer cell differentiation and accelerated proliferative activity” in lung cancer arising from emphysematous bullae.
Lung carcinoid tumors are quite rare, accounting for only 1% to 2% of all lung cancers.
In the most basic terms, there are calcified nodules and non-calcified nodules.
Calcified nodules contain deposits of calcium which are visible on imaging scans.
The finding of a SPN (Solitary Pulmonary Nodule)usually provokes a flurry of clinical and imaging activity as an SPN in an at-risk population is an alert signal of possible lung cancer. The frequency of malignant nodules in a given population is variable and depends on the endemicity of granulomatous disease. The percentage of malignant nodules also rises when dealing with at-risk populations. The problem is compounded by the fact that with the present generation of CT scanners, 1–2 mm nodules are discovered.
Calcification in a pulmonary nodule (PN) on imaging indicates a high probability that the lesion is benign. But not all calcified PN are benign and the differential considerations include a primary central lung carcinoid, metastasis, and a primary bronchogenic carcinoma. The widespread use of computed tomography (CT) has increased the sensitivity of detecting calcification in malignant tumors. Radiological demonstration of calcification in lung cancers is uncommon but when encountered may lead to misdiagnosis. Amorphous, punctate, and reticular patterns of calcification have been described in lung cancer. Malignant tumors may engulf a pre-existing granuloma, or tumor necrosis can manifest as tumor dystrophic calcification. Calcification in a mucinous adenocarcinoma may occur as a primary phenomenon. In a malignant PN, calcification appears in the form of larger lesions and is usually stippled or eccentric. To classify calcification in a benign PN certain criteria need to be fulfilled. Benign calcification should encompass over 10% of the PN and calcification should be central, diffuse, popcorn type, or laminated. To complicate matters malignant nodules may mimic the appearances of benign calcified granuloma... Six different patterns of calcification in a PN are known:
(I) central dense nidus
(II) diffuse solid
(III) laminated
(IV) popcorn
(V) punctate and
(VI) dendriform.
CT densitometry has been shown to have limited value when assessing spiculated nodules and its sensitivity (66%) and specificity (98%) for benign disease are not optimal.
Differential diagnosis of diffusely distributed small calcified nodules includes
infections,
lung metastases,
chronic pulmonary hemorrhage,
pneumoconiosis,
deposition diseases,
and idiopathic disorders such as pulmonary alveolar microlithiasis. It is imperative that before embarking on the workup of a high-density nodule that an extrinsic thoracic wall lesion is excluded.
Non-calcified nodules are classified as ground-glass opacities, partially solid or solid nodules. Ground glass opacities (GGO) look like a hazy (not clear) area
on a CT scan, like ground glass. This may be the result of inflammation caused by infection or other lung damage, but could also be a sign of a type of lung cancer that is slow-growing.
If the nodule grows, further testing may be needed to see if it is cancer.
By definition, a lung nodule is a rounded or irregular opacity, which may be well or poorly defined,
measuring ⩽3 cm in diameter, surrounded by aerated lung on radiological imaging.
With regard to SSNs, visual evaluation is a difficult task as nodule margins tend to be ill-defined and have
a low contrast concerning the surrounding lung parenchyma. In this context, uncertainties exist not
only in the nodule measurement, due to difficulties in delineating nodule margins and different
densitometric components of PSNs, but also in the classification of nodule morphological characteristics.
Chest CT with a mediastinal window and coronal reconstruction, showing calcifications affecting lymph nodes of several mediastinal and hilar chains. Note that several of them present calcifications predominantly in their periphery-“eggshell” calcifications.
Lymph node calcifications most often result from prior granulomatous infections, especially tuberculosis and histoplasmosis. Other, less common, causes are sarcoidosis, silicosis, amyloidosis, and calcifications secondary to the treatment of lymphomas (radiation therapy or chemotherapy). However, the patient in question had lymph node calcifications with characteristics that made them more specific. The calcifications involved lymph nodes of multiple chains, including some that presented eggshell calcifications.
When calcifications affecting multiple chains are observed, two diseases top the list of differential diagnoses: silicosis and sarcoidosis. Differentiation by imaging can be very difficult, because both diseases can present with small nodules, conglomerated masses, and areas of emphysema. It is therefore fundamental to investigate the clinical history of exposure to silica dust, given that most patients with silicosis have engaged in professional activities related to such exposure. Although a patient was a female and almost all cases of silicosis occur in male patients, she reported that she had been working at a lapidary, processing semiprecious stones, for 25 years. A diagnosis of silicosis was therefore made.
Silicosis is a chronic fibrotic lung disease caused by prolonged exposure to dust-containing free silica. The diagnosis of silicosis is based on the combination of a history of exposure to silica and characteristic findings on imaging tests. Mining, quarrying, drilling (wells, tunnels, and galleries), ceramics work, marble work, sandblasting, and artisanal work with semiprecious stones are all common professional activities in Brazil.
The classic radiological findings are small nodules, typically located in the posterior and upper lung regions, which can be disseminated through the lungs. The nodules can agglomerate, forming conglomerate masses. The most common lymph node involvement occurs in the form of calcifications in multiple lymph node chains. The past and present occupation of the patient is decisive for the final diagnosis of silicosis.
This is mentioned in my general discussion of lung cancer not my own findings.